무균 수막염(뇌막염)과 박테리아 수막염의 감별진단, Differential diagnosis of aseptic meningitis and bacterial meningitis
-
바이러스 수막감염, 그 외 비 화농 박테리아 수막 감염이나 다른 병원체 수막 감염, 또는 뇌막(수막) 중금속 중독 등으로 생긴 비 화농(고름) 수막염(뇌막염)을 무균 수막염(뇌막염)이라 한다.
-
대개의 박테리아 감염으로 생긴 수막염은 화농 수막염(뇌막염)이라 하고 결핵성 수막염 등 일부 박테리아 뇌막염은 비 화농 뇌막염은 무균성 수막염이라고도 한다.
-
수막 감염병(수막염)을 진단하는데 CBC 피 검사, ESR, C-반응 단백질 혈중농도, 프로칼시토닌(Procalcitonin/PCT) 정량검사, 그 외 혈액검사 등이 유용하게 사용되고 있다. 그 중 프로칼시토닌 정량검사가 가장 유용한 진단 가치가 있다고 한다.
-
프로칼시토닌은 칼시토닌(Calcitonin) 호르몬의 전구물질이고 갑상선의 C 세포에서 생성된다. 그러나 프로칼시토닌은 건강한 사람의 피 속에 있지 않는다.
-
심한 전신 감염병이 있을 때는 프로칼시토닌의 혈중 농도가 100ng이거나 그 이상 증가될 수 있다.
-
소아 뇌막염(수막염)의 5%는 박테리아 뇌막염이고 나머지는 무균 뇌막염이다.
-
소아 뇌막염이 생기면 피에서 프로칼시토닌 정량검사, C-반응 단백질, 백혈구 총수, 호중구 수 등을 검사하고 뇌척수 액을 뽑아 검사하는 것이 보통이다.
-
뇌척수 액에서 단백질 농도, 포도당 농도, 백혈구 수, 호중구 수, 그람 염색 현미경 세균검사, 박테리아 항원 등을 검사해서 무균 뇌막염에 걸렸는지 박테리아 뇌막염에 걸렸는지 감별 진단하는 것이 보통이다.
-
이상 설명한 여러 가지 검사결과 중 프로칼시토닌 정량검사의 결과치가 비정상적으로 증가되면 박테리아(성) 뇌막염에 걸려있다고 진단할 수 있다. 따라서 뇌막염에 걸렸을 때는 이 검사가 상당히 중요하다. 출처;ARCHIVES OF PEDIATRICS AND ADOLESCENT MEDICINE, DECEMBER 2008 p.1157.
수막염의 종류 Classification of Meningitis
|
뇌막염(수막염)의 종류 |
|
|
뇌막염을 일으킨 병원체의 종류에 따라, 비 병원체, 환자의 나이 등 따라 뇌막염을 다음과 같이 뇌막염을 분류 한다. |
박테리아 뇌막염, 바이러스 뇌막염, 곰팡이 뇌막염, 바이러스 뇌막염, 화학 물질 뇌막염 등 비 박테리아 감염으로 생기지 않은 뇌막염을 무균 뇌막염이라 한다. |
|
뇌막염이 급성, 만성, 아급성으로 생겼느냐에 따라 다음과 같이 뇌막염을 분류 한다 |
뇌막염이 급성으로 생기면 급성 뇌막염 만성으로 생기면 만성 뇌막염, 아급성으로 생기면 아급성 뇌막염이라 한다. |
|
뇌막염을 앓는 환자의 나이에 따라 뇌막염을 다음과 같이 분류 한다. |
신생아에게 생긴 뇌막염은 신생아 뇌막염, 신생아기 이후 아이들에게 생긴 뇌막염을 소아 뇌막염, 성인들에게 생기는 뇌막염 |
|
바이러스 감염으로 생기는 바이러스 뇌막염을 다음과 같이 분류 한다. 바이러스 뇌막염(수막염)도 무균성 뇌막염(수막염)으로 취급될 수 있다. |
장 바이러스 뇌막염, 폴리오바이러스 뇌막염, 콕삭키바이러스 뇌막염, 에코바이러스 뇌막염 헤르피스 단순 포진 바이러스 뇌막염, 사람 면역 결핍 바이러스 뇌막염,, 유행성 이하선염 바이러 뇌막염, 서 나일 바이러스 뇌막염, 일본 뇌염 바이러스 뇌막염, 아데노바이러스 뇌막염, 아보바이러스 뇌막염, 엡스타인–바바이러스 뇌막염, 파라인플루엔자바이러스 뇌막염, 그 외 바이러스 뇌막염 |
|
뇌막염을 일으킨 박테리아의 종류에 따라 박테리아 뇌막염을 다음과 같이 분류한다. |
히브 균 뇌막염, 수막구균 뇌막염(수막구균 수막염), 살모넬라균 뇌막염, 포도상구균 뇌막염, 폐렴 연쇄구균 뇌막염, 결핵균 뇌막염 리스테리아 모노사이게너스 뇌막염 Kigella kingae 뇌막염, 탄저병 뇌막염, 스트렙토 배실러스균 뇌막염, 황색포도상구균 뇌막염, 비 A군 비 B군 연쇄상구균 뇌막염, 에리시나균 뇌막염, 캄필로박터균 뇌막염, 라이병 뇌막염, 아나플라스마(Anaplasma) 뇌막염, Bacillus anthracis 뇌막염, Coxiella burnetii 뇌막염, 대장균 뇌막염, 그 외 박테리아 뇌막염 |
|
비병원체 염증으로 인해 생긴 뇌막염을 무균 뇌막염 또는 무균 수막염(Aseptic meningitis)에 속 한다. 원인에 따라 무균 뇌막염(수막염)을 다음과 같이 분류한다. |
납중독 뇌막염, 화학물질 뇌막염, 백혈병 뇌막염, 호산구 뇌막염, 약물 뇌막염, 알레르기 뇌막염 그 외 뇌막염 |
|
불완전 치료 화농성 뇌막염 Partially treated pyogenic meningitis |
박테리아 뇌막염을 앓고 있는데 뇌막염이 아닌 다른 감염병을 앓고 있다고 추정으로 진단하고 추정 진단에 따른 감염병을 치료한 경우, 즉 박테리아 뇌막염에 대한 치료를 하지 않거나, 박테리아 뇌막염을 앓고 있다고 확실히 진단 한 후 그 박테리아 뇌막염을 적절히 치료하지 안 해 박테리아 뇌막염이 완치되지 않거나 완전히 치료되지 않은 박테리아 뇌막염을 더 이상 치료하지 않으면 뇌막염을 일으킨 박테리아가 계속 뇌막 감염병을 일으켜 뇌막염이 완치되지 않은 경우. 박테리아 뇌막염의 전형적인 증상 징후가 나타나지 않을 수 있지만 그 뇌막염이 아급성 뇌막염으로 이어 질 수 있다. 이런 종류의 박테리아 뇌막염을 “불완전 치료 화농 뇌막염” 또는 불완전 치료 세균 뇌막염이라고 한다. |
불완전 치료 화농 수막염 Partially treated pyogenic meningitis
-
박테리아 뇌막염을 앓고 있는 것을 확실한 진단을 붙이지 않은 상황에서 뇌막염이 아닌 다른 감염병으로 추정 진단하고 추정으로 진단한 감염병을 치료한 경우, 즉 박테리아 뇌막염에 대한 치료를 하지 않거나,
-
또는 박테리아 뇌막염을 확실히 진단을 한 후 그 박테리아 뇌막염을 적절히 치료하지 않은 경우 박테리아 뇌막염이 완치되지 않을 수 있다.
-
또한 완전히 치료되지 않은 상태에서 그 박테리아 뇌막염을 더 이상 치료하지 않으면 그 박테리아 뇌막염을 일으킨 박테리아가 다시 뇌막에 감염되어 박테리아 뇌막염이 다시 재발될 수 있다.
-
이때 박테리아 뇌막염의 전형적인 증상 징후가 나타나지 않을 수 있지만 그 뇌막염이 아급성 뇌막염으로 이어 질 수 있다.
-
이런 종류의 박테리아 뇌막염을 “불완전 치료 화농 뇌막염” 또는 불완전하게 치료된 세균 뇌막염이라고 한다. 이때도 비 화농 수막염 샅태로 될 수 있다.
수막염의 증상 징후

사진 2-62. 피 피검 물을 채취해 CBC 피 검사, 혈액 전해질 농도 검사, 혈액 세균 배양 검사 등을 해서 진단하는데 도움 얻는다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
-
뇌막염이 급성으로 시작했느냐, 또는 만성으로 시작했느냐, 뇌막염이 박테리아 감염으로 생겼느냐, 바이러스 감염으로 생겼느냐, 곰팡이 감염으로, 또는 화학물질 중독 등으로 생겼느냐에 따라 증상 징후가 다르다.
-
뇌막염을 일으킨 박테리아의 종류나 바이러스의 종류에 따라 뇌막염의 증상 징후가 다르다.
-
결핵균 뇌막염(수막염), 폐렴연쇄구균 뇌막염, 수막구균 뇌막염, 히브 박테리아 뇌막염 등의 증상 징후는 원인 병원체의 종류에 따라 다르다.
-
신생아 뇌막염의 증상 징후는 신생아기 이후 소아청소년 뇌막염의 증상 징후가 다르다.
-
뇌막염의 초기의 증상 징후와 많이 진행된 뇌막염의 증상 징후나 뇌막염의 말기의 증상 징후가 다르다.
-
뇌막염만 있을 때의 증상 징후와 뇌막염와 패혈증 등 합병증이 있을 때와 없을 때의 증상 징후가 다르다.
-
박테리아 뇌막염의 증상 징후는 다음과 같다.
-
박테리아 뇌막염이 있으면 심한 두통, 구토, 고열 등의 증상 징후가 거의 일률적으로 나타난다.
-
독성 상태에 빠진다.
-
그 외 신경이 예민하고 잠을 비정상적으로 많이 자고 입맛이 없고 탈진되고
-
탈수,
-
경련, 뇌신경마비,
-
혼수, 쇼크 등에 빠질 수 있다.
-
이런 증상 징후가 나타나기 전에 감기나 인두염 등 바이러스 상기도 감염병을 며칠 동안 앓는 경우도 있고
-
그런 바이러스 상기도 감염병으로 콧물, 인두 통, 근육통, 열, 기침 등의 증상 징후가 뇌막염의 증상 징후가 나타나기 전 보다 더 일찍 나타날 수 있다.
-
중이염, 축농증, 후두염, 폐렴 등의 감염병을 일으킨 박테리아가 뇌막에 감염되어 박테리아 성 뇌막염이 생길 수 있다.
-
수막염의 진단
-
병력, 증상 징후, 진찰소견 등을 종합해서 뇌막염이 의심되면 요추천자 뇌척수 액 검사를 한다.
-
그람 현미경 뇌척수 액 세균검사 등으로 뇌막염을 일으킨 박테리아를 찾아내고
-
뇌척수 액 세균 배양검사,
-
뇌척수 액 포도당 농도, 단백 농도, 백혈구 수치와 백혈구 종류의 감별계산,
-
적혈구수치, 백혈구의 종류 등을 검사하고
-
소변, 혈액, 대변 등으로 세균 배양 검사 등을 해서 진단한다.
-
필요에 따라 가슴 X선 검사와 뇌 MRI 검사 등으로 진단한다.
요추천자 뇌척수 액 검사 전 수막염을 항생제로 치료 했을 때
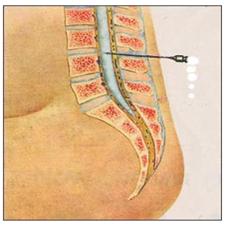
그림 2-63. 뇌염이나 뇌막염이 의심되면 요추 천자 뇌척수 액을 뽑아 뇌척수 액의 단백 농도, 뇌척수 액의 당 농도, 뇌척수 액 적혈구 수, 백혈구 수, 뇌척수 액 그람 염색 현미경 세균검사, 뇌척수 액 세균배양 검사 등으로 뇌염이나 뇌막염을 진단한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
-
소아가 세균성 뇌막염응 앓고 있는 중 요추천자 (Spinal tap/Lumbar puncture) 뇌척수 액 검사를 하지 않고 뇌막을 통과해서 뇌 척수 액 속으로 들어 갈 수 있는 Ceftriaxone 등 경구용 항생제나 주사용 항생제로 뇌막염을 치료받은 후, 요추천자 뇌척수 액 피검물 검사 결과에 관한 연구.
-
뇌척수 액의 단백질 농도가 감소되었고
-
뇌척수 액의 포도당 농도가 증가되었고
-
뇌척수 액 세균 배양 검사 결과가 음성으로 나타나는 비율이 높았고.
-
그러나 요추천자 뇌척수 액을 검사하기 전 뇌막을 통과해서 뇌척수 액 속까지 도달할 수 없는 Cephalexin제나 Azithromycin제 등 항생제로 치료받은 경우 뇌척수 액 단백질 농도와 포도당의 농도는 위에서 설명한 결과가 생기지 않았다고 한다.
-
일부 치료 세균성 뇌막염(불완전하게 치료된 화농성 뇌막염)의 진단 치료에 참고가 될 수 있는 재료이다. 출처;Infectious Diseases in children 10/2008
프로칼시토닌 정량검사와 무균 수막염과 박테리아 수막염
-
바이러스 감염, 그 외 비 박테리아 병원체 감염, 중금속 중독 등으로 생긴 뇌막염은 무균 뇌막염에 속한다.
-
박테리아 뇌막염(Bacterial meningitis)은 박테리아 감염으로 생긴다.
-
프로칼시토닌(Procalcitonin/PCT)의 정량검사가 감염병을 감별 진단할 때 유용하게 쓰이고 있다.
-
프로칼시토닌(Procalcitonin)은 칼시토닌(Calcitonin) 호르몬의 전구물질이고 갑상선의 C 세포에서 생성된다.
-
프로칼시토닌은 건강한 사람의 혈액 속 있지 않는 것이 정상이다.
-
그러나 전신 감염병을 심하게 앓고 있을 때는 혈 중 프로칼시토닌의 농도가 100ng 이상으로 증가될 수 있다.
-
소아청소년 수막염(뇌막염)의 5%는 박테리아 뇌막염이고 나머지는 무균 뇌막염이다.
-
소아청소년에게 뇌막염이 생기면
-
혈 중 프로칼시토닌 정량을 검사 하고,
-
C 반응성 단백질(C-reactive protein/CRP)(p.000 참조),
-
백혈구 총수 검사,
-
호중구 수 검사 등을 하고
-
뇌척수 액으로 단백질 농도, 포도당 농도, 백혈구 수, 호중구 수, 그람 염색 현미경 세균검사, 박테리아 항원 검사, 세균 배양 검사 등을 해서 무균 뇌막염과 박테리아 뇌막염을 감별진단 한다.
-
이상 설명한 여러 가지 임상 검사 결과 중 프로칼시토닌 정량 검사 치가 비 정상적으로 증가되면 박테리아(성) 뇌막염에 걸렸다고 진단할 수 있다. 출처; ARCHIVES OF PEDIATRICS AND ADOLESCENT MEDICINE, DECEMBER 2008 p.1157.
표 2-3. 뇌 척수액 검사로 수막염(뇌막염)을 감별 진단할 수 있다. Differential diagnosis of meningitis by cerebrospinal fluid examination
|
백혈구 수, 포도당 농도, 단백질 농도 세균검사→ 뇌막염 의 종류↓ |
뇌 척수 액 백혈구 수 |
뇌 척수 액 포도당 농도 |
뇌 척수 액 단백질 농도 |
뇌 척수 액 세균그람 염색 |
뇌 척수 액 세균 배양 |
|
정상 뇌 척수액 검사 |
0-2 림프구mm3 |
40mg% 이상 |
40mg% 이하 |
– |
– |
|
화농성 뇌막염(화농성 뇌수막염) |
200-5000mm3,대부분 다형 핵구 |
감소 |
증가 |
+ |
+ |
|
불완전 치료된 세균성 뇌막염 |
화농성 뇌막염(뇌수막염)과 거의 같거나 림프구 수가 증가할 수 있다. |
감소 |
증가 |
± |
± |
|
육아종성 뇌막염 |
100-300mm3,대부분이 림프구 |
감소 |
증가 |
– |
+ |
|
무균 뇌막염 |
100-700mm3,50%이상이 림프구 |
정상 |
정상이거나 증가 |
– |
– |
출처; Quick reference to Pediatric Emergency, JB Lippincott Company, p.246
Differential diagnosis of aseptic meningitis and bacterial meningitis
• Non-purulent (pus) meningitis (meningitis) caused by viral meningitis, other non-purulent bacterial meningeal infections or other pathogenic meningeal infections, or meningeal (meninges) heavy metal poisoning is called aseptic meningitis (meningitis).
• Meningitis, most often caused by a bacterial infection, is called suppurative meningitis (meningitis), while some bacterial meningitis, such as tuberculous meningitis, is called aseptic meningitis, and non-purulent meningitis.
• CBC blood test, ESR, C-reactive protein blood concentration, procalcitonin (PCT) quantitative test, and other blood tests are useful for diagnosing meningeal infectious disease (meningitis). Among them, procalcitonin quantitative test is said to have the most useful diagnostic value.
• Procalcitonin is a precursor of the hormone Calcitonin and is produced by C cells of the thyroid gland. However, procalcitonin is not in the blood of healthy people.
• In the presence of severe systemic infectious diseases, procalcitonin blood levels may be increased to 100 ng or more.
• 5% of pediatric meningitis (meningitis) is bacterial meningitis and the remainder is aseptic meningitis. • When pediatric meningitis develops, it is common to test for procalcitonin quantitative test, C-reactive protein, total white blood cell count, and neutrophil count from blood, and to draw and test cerebrospinal fluid.
• Differential diagnosis of aseptic or bacterial meningitis is usually done by testing the cerebrospinal fluid for protein concentration, glucose concentration, white blood cell count, neutrophil count, Gram-stained microscopic bacteriology, and bacterial antigen.
• Among the various test results described above, if the result of the quantitative procalcitonin test is abnormally increased, it can be diagnosed as having bacterial (sex) meningitis. Therefore, this test is very important when you have meningitis. Source: ARCHIVES OF PEDIATRICS AND ADOLESCENT MEDICINE, DECEMBER 2008 p.1157.
Classification of Meningitis
|
Types of meningitis (meningitis) |
|
|
According to the type of pathogen that caused meningitis, non-pathogen, and the age of the patient, meningitis is classified as follows: |
• bacterial meningitis; • viral meningitis; • fungal meningitis; • Meningitis that does not result from a non-bacterial infection, such as viral meningitis or chemical meningitis, is called aseptic meningitis. |
|
Meningitis is classified according to whether it is acute, chronic, or subacute. |
If meningitis develops acutely, acute meningitis If chronic, chronic meningitis, If it is subacute, it is called subacute meningitis. |
|
According to the age of the patient with meningitis, meningitis is classified as follows: |
Neonatal meningitis, neonatal meningitis, Meningitis in children after neonatal period, juvenile meningitis, meningitis in adults |
|
Viral meningitis caused by viral infection is classified as follows: Viral meningitis (meningitis) can also be treated as aseptic meningitis (meningitis). |
|
|
Depending on the type of bacteria that causes meningitis, bacterial meningitis is classified as follows: |
• Mycobacterium tuberculosis meningitis • Listeria monocygenus meningitis • Kigella kingae meningitis; • Anthrax meningitis; • Streptococcus meningitis; • Staphylococcus aureus meningitis; • non-group A non-group B streptococcal meningitis; • ericina meningitis; • Campylobacter meningitis; • Reye’s disease meningitis; • Anaplasma meningitis; • Bacillus anthracis meningitis; • Coxiella burnetii meningitis; • Escherichia coli meningitis; • Other bacterial meningitis |
| Meningitis caused by non-pathogenic inflammation is classified as aseptic meningitis or aseptic meningitis. According to the cause, aseptic meningitis (meningitis) is classified as follows: |
lead poisoning meningitis, chemical meningitis, leukemia meningitis, eosinophilic meningitis, drug meningitis, allergic meningitis other meningitis |
|
Partially treated pyogenic meningitis |
• If you have bacterial meningitis, presumptive diagnosis that you have an infectious disease other than meningitis and treated for an infectious disease according to the presumptive diagnosis, that is, no treatment for bacterial meningitis; • Bacterial meningitis cannot be cured or cured by not treating the bacterial meningitis properly after a definitive diagnosis has been made. • If untreated bacterial meningitis is no longer treated, the bacteria that caused meningitis continue to cause meningeal infections and meningitis is not cured. • The typical symptoms of bacterial meningitis may not appear, but the meningitis can lead to subacute meningitis. This type of bacterial meningitis is called “incompletely cured suppurative meningitis” or incompletely cured bacterial meningitis. |
Partially treated pyogenic meningitis
• If a presumptive diagnosis of an infectious disease other than meningitis is presumptive and treatment of the presumptively diagnosed infectious disease, that is, no treatment for bacterial meningitis, in the absence of a definitive diagnosis of bacterial meningitis;
• Alternatively, bacterial meningitis may not be cured if it is not properly treated after a definitive diagnosis of bacterial meningitis.
• In addition, if the bacterial meningitis is no longer treated in the absence of complete treatment, the bacteria that caused the bacterial meningitis can re-infect the meninges and cause the bacterial meningitis to recur.
• The typical symptoms of bacterial meningitis may not appear at this time, but the meningitis can lead to subacute meningitis.
• This type of bacterial meningitis is called “incompletely cured suppurative meningitis” or incompletely cured bacterial meningitis. It can also become non-purulent meningitis.
Signs of symptoms of meningitis
Picture 2-62. Blood samples are collected and CBC blood test, blood electrolyte concentration test, blood bacterial culture test, etc. are performed to help diagnose. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Symptoms vary depending on whether the meningitis has an acute or chronic onset, whether the meningitis is caused by a bacterial infection, a viral infection, a fungal infection, or a chemical poisoning.
• Symptoms of meningitis differ depending on the type of bacteria or virus that caused the meningitis.
• Symptoms of Mycobacterium tuberculosis meningitis (meningitis), streptococcal meningitis pneumococcal meningitis, meningococcal meningitis, and Heb-bacterial meningitis depend on the type of pathogen.
• Symptomatic signs of neonatal meningitis differ from those of juvenile meningitis after the neonatal period.
• The early symptoms of meningitis are different from those of advanced meningitis or the late stages of meningitis.
• Symptom signs with meningitis alone are different from those with and without complications such as meningitis and sepsis.
• Symptoms of bacterial meningitis include: o With bacterial meningitis, symptoms such as severe headache, vomiting, and high fever appear almost uniformly.
o Become toxic.
o Others are nervous, sleep abnormally, have no appetite, and are exhausted. o Dehydration;
o Convulsions, cranial nerve palsy,
o You may fall into a coma or shock. o You may have a viral upper respiratory infection such as a cold or pharyngitis for several days before these symptoms appear.
o With such viral upper respiratory infections, symptoms such as runny nose, sore throat, muscle pain, fever, and cough may appear earlier than before symptoms of meningitis appear.
o Bacteria that cause infectious diseases such as otitis media, sinusitis, laryngitis, and pneumonia can infect the meninges and cause bacterial meningitis.
Diagnosis of meningitis
• If meningitis is suspected based on the medical history, symptom signs, and examination findings, a lumbar puncture cerebrospinal fluid test is performed.
• Gram microscopic cerebrospinal fluid bacteriological examination, etc. to find out the bacteria that caused meningitis
• cerebrospinal fluid bacterial cultures;
• Differential calculation of cerebrospinal fluid glucose concentration, protein concentration, leukocyte count and leukocyte type;
\• Check the red blood cell count, white blood cell type, etc.
• Diagnosis is made by performing a bacterial culture test with urine, blood, and feces.
• Diagnosis is made by chest X-ray examination and brain MRI examination, if necessary. When meningitis was treated with antibiotics before lumbar puncture cerebrospinal fluid test
Figure 2-63. If encephalitis or meningitis is suspected, lumbar puncture cerebrospinal fluid is drawn, and cerebrospinal fluid protein concentration, cerebrospinal fluid sugar concentration, cerebrospinal fluid red blood cell count, white blood cell count, cerebrospinal fluid Gram stain microscopic bacteriological test, cerebrospinal fluid culture test, etc. to diagnose Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Spinal tap/Lumbar puncture in children suffering from bacterial meningitis. Treatment of meningitis with oral or injectable antibiotics such as Ceftriaxone, which can pass through the meninges and enter the cerebrospinal fluid without cerebrospinal fluid examination. After receiving, a study on the results of the lumbar puncture cerebrospinal fluid specimen test. • decreased protein concentration in cerebrospinal fluid;
• The glucose concentration in the cerebrospinal fluid was increased and
• There was a high rate of negative cerebrospinal fluid culture test results.
• However, before the lumbar puncture cerebrospinal fluid test, if the cephalexin or azithromycin was treated with antibiotics such as cephalexin or azithromycin, which cannot reach the cerebrospinal fluid through the meninges, the cerebrospinal fluid protein concentration and glucose concentration did not produce the results described above.
• Some therapeutic materials may be used as a reference in the diagnostic treatment of bacterial meningitis (incompletely treated suppurative meningitis). Source: Infectious Diseases in children 10/2008 Procalcitonin quantitative test and aseptic meningitis and bacterial meningitis
• Meningitis caused by viral infection, infection with other non-bacterial pathogens, or heavy metal poisoning is classified as aseptic meningitis.
• Bacterial meningitis is caused by a bacterial infection.
• Quantitative testing of procalcitonin (PCT) is useful for differential diagnosis of infectious diseases.
• Procalcitonin (Procalcitonin) is a precursor of the hormone Calcitonin and is produced by C cells of the thyroid gland.
• It is normal that procalcitonin is not in the blood of a healthy person.
• However, the concentration of procalcitonin in the blood may increase to 100 ng or more when a person is severely ill with a systemic infectious disease.
• 5% of pediatric meningitis (meningitis) is bacterial meningitis and the remainder is aseptic meningitis.
• If a child or adolescent develops meningitis
• Test the amount of procalcitonin in the blood;
• C-reactive protein (CRP) ;
• white blood cell count,
• Doing a neutrophil count test, etc.
• Differential diagnosis of aseptic meningitis and bacterial meningitis is performed by cerebrospinal fluid, protein concentration, glucose concentration, white blood cell count, neutrophil count, Gram-stained microscopic bacteriology, bacterial antigen test, and bacterial culture test.
• If the quantitative test of procalcitonin is abnormally increased among the results of various clinical tests described above, it can be diagnosed as having bacterial (sexual) meningitis. source; ARCHIVES OF PEDIATRICS AND ADOLESCENT MEDICINE, DECEMBER 2008 p.1157
표 2-3. Differential diagnosis of meningitis by cerebrospinal fluid examination
| white blood cell count, glucose concentration, protein concentration Bacterial test→ meningitis Kind of ↓ |
Cerebrospinal fluid white blood cell count |
Cerebrospinal fluid glucose concentration |
Cerebrospinal fluid protein concentration |
Cerebrospinal fluid bacterial gram staining |
Cerebrospinal fluid bacterial culture |
|
Normal cerebrospinal fluid test |
0-2 lymphocytes mm3 |
40mg% or more |
40mg% or less |
– |
– |
|
Purulent meningitis (purulent meningitis) |
200-5000mm3, mostly polymorphic nucleolus spheres |
decrease |
increase |
+ |
+ |
|
Incompletely treated bacterial meningitis |
It may be about the same as purulent meningitis (meningitis) or an increased number of lymphocytes. |
decrease |
increase |
± |
± |
|
granulomatous meningitis |
100-300mm3, mostly lymphocytes |
decrease |
increase |
– |
+ |
|
aseptic meningitis |
100-700mm3,50% or more are lymphocytes |
normal |
normal- increase |
– |
– |
A quick reference to Pediatric Emergency, JB Lippincott Company, p.246
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- Emergency Pediatrics, A guide to ambulatory care, 5th ed Roger M. Barkin, Peter Rosen, p.548
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey grant, and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Manual of Emergency Care
- 소아가정간호백과-부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Nelson Textbook of Pediatrics 14th ed. Beherman,
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
- Red book 29th-31st Ed 2021
- Nelson Text Book of Pediatrics 19th-21st Edition
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- Growth and Development of Children, George H. Lowrey 8th edition
- 소아과학 대한교과서
- 제1권 소아청소년 응급의료 참조문헌과 출처
- Other
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.